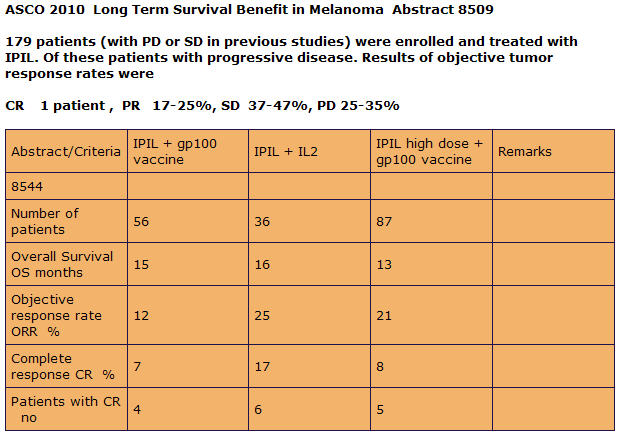
Jim,
First of all thank you for replying to my post. I usually don’t get many replies. When I talk to my wife about this, within the first five minutes she is telling me “I am loosing her.” It has taken me close to three years to get to where my knowledge on melanoma and the immune system is today. I don’t mean to talk over patient heads. It is just the scientist in me. I worked at Eastman Kodak’s Research laboratories for 25 years.
Now to answer you first question:You have said that the most effective durable treatment for advanced melanoma would consist of Ipilimumab combined with IL2 - is that correct?
Based on my research today, IL-2 and Anti-CTLA-4 (Ipilimumab) are most durable as we speak. A new phase I therapy is showing great promise with less side effects. That is anti-PD-1 Therapy. These therapies don’t need a specific HLA type to get into the trials.
There is also a very, very ,very new therapy that is still in translational stage. Translational research is a way of thinking about and conducting scientific research to make the results of research applicable to the population under study and is practised in the natural and biological, behavioural, and social sciences. It is usally conduted with animals like rats, mice, monkeys.

Anyway this therapy combines the Anti-CTLA-4 and Anti-PD-1. It has shown synergistic results.

If you have c-Kit or BRAF mutations, then targeted therapy may used but may not be durable.
If you are HLA-02 Positive, You have the option of ACT therapy with Dr. Rosenberg or Dr. Patrick Hwu at NCI or MD Anderson. They have gotten 72 % response rate with I think about 36 % complete response is I am not mistaken.
Second Question:There are no studies currently availble that combine Ipi and IL2, is that correct?
Define combine? There was a clinical study done by Dr. Rosenberg and colleages.

As you can see in the graph above, IL-2 was added prior to the maximum propagation of the CD4+ T helper cells. IL-2 is known as a growth factor. So what I believe happened in this trial, they grew the Tregs.
IL-2 treatment during the expansion phase was detrimental to the survival of rapidly dividing effector T cells. In contrast, IL-2 therapy was highly beneficial during the death phase, resulting in increased proliferation and survival of Tumor-specific T cells. IL-2 treatment also increased proliferation of resting memory T cells in the host that controlled the disease. A tumor-specific T cell in chronically infected Host also responds to IL-2 resulting in decreased tumor burden. Thus, timing of IL-2 administration and differentiation status of the T cell are critical parameters in designing IL-2 therapies (Blattman et al., 2003).
So what I am trying to say is you do the Ipilimumab therapy first. Wash out for about 50 days, and then start IL-2 Therapy.
Take away: It is a systemic combination with dosing and timing involved. Systemic Combinatorial Therapy.
Question 3:If someone were to choose to do a combination treatment on their own (i.e. get IL2 following a course of Ipi through one of the clinical trials), would there be an advantage
to starting IL2 as soon as possible after stopping Ipi? Is there a time frame after which there would be no advantage to having received Ipi prior to taking IL2?
Base on papers from ITOH etal and others, 49 days after activation is at the maximum growth phase for the CD8- T-cells that mature into Cytotic T Lymphocytes.
Results: Graph setupKinetic Study of rIL-2-induced Expansion. In all 12 metastatic melanomas tested, a substantial proportion of TIL was present in tumor cell suspensions.
The ratio of lymphocytes to tumor cells ranged from 0.03 to 1.25 with an average ratio of 0.40 t 0.37. By fluorescence analysis,
TIL consisted of 78 days 11% CD3
T cells, 33 days 10% CD4+
T cells, 49 days 17% CD8+Their CD4/CD8 ratio was 0.67.
(ITOH et al., 1988)
It was also reported that there is a time factor involved.
Our results show that T4 + human T cells differ substantially from T8 + cells with respect to their IL-2 responsiveness. T4 + cells cease to proliferate well before T8 + cells during a primary response. (GULLBERG AND SMITH et al.,1986)
Is there a time frame after which there would be no advantage to having received Ipi prior to taking IL2?Yes, Ipilimumab has a half life of 15 days. So say you get one dose at 3.0 mg/Kg.
Days-- concentration
0-- 3
15-- 1.5
30-- 0.75
45-- 0.375
60-- 0.1875
75-- 0.09375
90-- 0.04687
105-- 0.02343
120-- 0.01171
135-- 0.00587
150-- 0.00292
165-- 0.00146
180-- 0.00073
It gets more complicated when you get multiple doses. Four dose regiment.
Days-- concentration
0-- 3
15-- 1.5
30-- 3.7
45-- 4.85
60-- 5.425
75-- 2.7125
90-- 1.35625
105-- 0.68
120-- 0.34
135-- 0.17
150-- 0.08
165-- 0.04
180-- 0.021
I am not sure where the limited threshold is but, at day 49 you have close to the maximum concentration of Ipilimumab in your body.
Since I used Tremelimumab with Half Life = 21 days and did 15mg/Kg
I had at day 50 approximately 2.17 mg/Kg anti-CTLA-4 level in my body
If I had to venture an educational guess, I would say after a four dose regime, you have 75 days to do the HD IL-2.To back this theory up, we will use a chart from Dr. Wolchok experience the Ipilimumab.
It is a chart with the Absolute Lymphocyte count. (ALC). It is the CD4+ T-cells and CD8+ T cells combined.

As you can see from the graph, the maximum ALC was about week 7.
Week seven correlates to 49 days. That is when CD8+ T cells are at their maximum growth.
Question 4:Last, is there any evidence that IL2's efficacy is enhanced by combining it with other agents (i.e. Biochemotherapy), either with or without first receiving Ipi?
This my take on the situation. You need the
tumor-specific antigen to presented to the T-cells as signal 1. That could be a vaccine, radiation therapy or chemo to shed the antigen.
Secondly you need the costimulation of the CD28/B7 interface. By using Ipilimumab that blocks the CTLA-4 receptor from binding to the B7 molecule and shutting down the response.
Anti-CTLA-4 (ipilimumab) also blocks the CTLA-4 receptor on the Treg cells subduing their surpress function.
Third you need a
“Danger Signal” to get the cell to migrate to the tumor site. This may be done with inflammatory Cytokines like IL2, IL17, IL-1,IL-12,IFN gamma that act directly on the T-cells. This signal was found to optimally activate the Th1 differentiation and lead to the clonal expansion of the T-cells.
It has come to light recently that Ipilimumab helps also in the differentiation by tilting the balance towards Th17 cells. These cells secrete IL-17 which recruite the neutrophils. This all takes place at the tumor’s microenviroment. The neutrophils secrete chemokines that are chemoattractants.
These chemokines, MIP-1alpha, MIP-1beta, and MCP-1 are recently reported to serve as chemoattractants for Th1 cells. MIP-1alpha and MCP-1 are also reported to enhance antigen-specific (CTL) Cytotoxic T Lymphocyte induction. Studies revealed that MIP-1alpha /beta released from neutrophils are involved in recruitment of macrophages, T cells, monocytes, dendritic cells (DC), neutrophils and NK cells.
MIP-1 attracts predominantly CD8+ T cells while MIP-1 attracts CD4+ cells, although there is some overlap between subsets in response to both chemokines.
The other Chemokine MCP-1, binds to CCR2 to accumulate monocytes/macrophages, DC, T cells, and NK cells, thereby playing an important role in innate and adaptive immunity. CCR2 is Chemokine receptor that is key determinant of leucocyte trafficking.
IL-2 strongly upregulates expression of CCR2. With the MCP-1/CCR2 interface, the cells can traffic towards the tumor’s microenvironment. The trafficking of the cells and inflammatory cytokines present the perfect storm in the tumor’s microenvironment to induce the right immune response to eradicate the cancer, Melanoma.
So to answer your question, is there any evidence that IL2's efficacy is enhanced by combining it with other agents (i.e. Biochemotherapy), either with or without first receiving Ipi? yes if you know and take a systemic approach. You need to activate the t-cells before introducing IL-2. IL-2 can be the activator for small patient population.
As for Ipilimumab going it alone, like IL-2 can be the activator for small patient population. But when you do a systematic combinatorial therapy, there can be a synergetic result, complete response.
I hope I answered you questions, and please don’t hesitate to ask them. I do all this time by requesting reseach papers from around the world. Each question is a learning tool. There are no stupid questions. Knowledge is power to make an educated decision. Your Life may depend on it. There are many paths to take. Just follow the yellow brick road to complete response.
“It is not the strongest of the species that survives, nor the most intelligent, but the one most responsive to change.”
~Charles Darwin~
Take Care,
Jimmy B